I have been using Electronic Health Records now for over 10 years. Like most physicians who have used EHRs, I would not ever go back to a paper-based medical record.
Having said that, it is important to recognize some of the potential problems created by some EHR products. One potential pitfall of some EHRs is the number of steps it takes to find information that is in the system. Yes, it may be easier to find than in an old paper-based system but it is still far from ideal. Also there is a lot more information that is accessible.
To illustrate my point, let take a hypothetical scenario that most physicians will recognize from real life.
You are working in a hospital and you note that one of your patients has anemia on the complete blood count test. Reported along with the hemoglobin are some other important numbers like the average size of the red blood cells. This helps to narrow down the list of causes of his anemia. One would of course want to make sure from the patient if there is history of this condition or of bleeding. In addition usually you would need more data from the EHR e.g.
- Previous levels of hemoglobin
- A trend of hemoglobin values over several years
- Previous work-ups for anemia like reticulocyte counts, iron studies, vitamin b12 levels etc.
- Previous investigations for bleeding sources e.g. endoscopy or colonoscopy where appropriate.
- Notes from previous consultations with a hematologist
This information tends to be quite fragmented in the EHRs which are often organized under categories like lab results, radiology, cardiology, notes, etc. Reports of a colonoscopy procedure may be found under the notes section and the results of the biopsy done during the colonoscopy may be under the lab results section with no hyperlink between the two. Recommendations from the gastroenterologist who did the colonoscopy may be found under the letter to patient section. Collecting this information from the EHR can take a lot of mouse clicks and several minutes depending on the user interface and various hardware, software, database and networking variables. This is time well-spent as this information can give one a diagnosis or at least guide our approach to care.
Unfortunately, this is usually only one of several issues that this patient might have. He could have an abnormal kidney function test, a low level of sodium, an abnormality on the chest x-ray (with radiologist recommending a CT scan), a question of a prior heart attack on the EKG etc. Tracking down each of these thoroughly could take a significant amount of time.
To complicate matters the EHRs may be fragmented between inpatient and outpatient areas requiring additional work to access the ambulatory records.
As all this time starts adding up, it may be quite tempting for providers to simply reorder a set of tests for working up the anemia rather than look up the prior information. This process is made simpler due to "Order sets" that are available in EHRs to make test ordering easier and standardized. Thus with a couple of clicks you can reorder all the tests and await the results.
One of the potential benefits of EHRs is to prevent duplicate test ordering. Unfortunately unless we develop ways for providers to more easily review data in a meaningful manner, this dream may not be realized. The worst part of this scenario is that as providers order more tests, we have more data to review thus perpetuating the information overload.
So what are the possible solutions?
- Contextually appropriate menus -e.g right click on an abnormal test result to get prior test results.
- Data visualization tools that can generate graphs of trends and associated factors with one click. While most EHRs have graphing tools, it takes several steps (selecting data range, tests etc) to generate these.
- Built-in review sets - If we can have order sets for ordering related sets of tests, we can easily develop review sets for looking up test results and make these built-in. Some EHRs allow providers to create these filters or review sets but a lot of physicians are unaware of this functionality.
- Have a view that is based on issues rather than dates. Thus just like your e-mail client's conversation view, would it not be easier to see a patients problem list and then click on a problem to see all tests, notes, letters etc related to that problem? Yes it would take some time to tag each item with the problem but the returns would be well worth it.
- Have a mechanism for capturing the time spent reviewing data and automatically documenting a summary of the data reviewed with hyperlinks to the data in the visit note. Presently physicians have to document what they reviewed by typing/dictating/copy-pasting into their notes. This is an inefficient process which could be improved. This will help the physician by saving time and also allow for billing using the time code.
- Dr. Watson and Siri? Allow the Watson system to analyze the patient's EHR and then allow querying of the database using a Siri-like voice recognition and natural language processing.
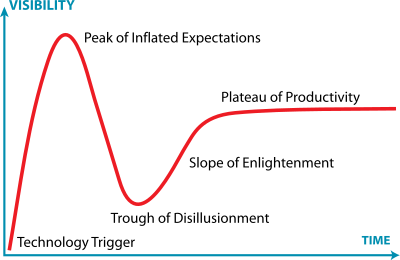 |
| The Hype Cycle from Gartner |
EHRs may be going through a peak of inflated expectations or the trough of disillusionment depending on your point of view (See Hype Cycle in Wikipedia). As we start applying innovative technology to EHRs we should soon (hopefully) be on the slope of enlightenment that will help realize their full potential.
